The Screaming
I heard the screaming before I even reached the ER's main corridor. It wasn't the usual sounds you get used to in emergency medicine—the groans, the confused elderly patients calling for help, the occasional drunk college kid. This was different. Raw. Desperate. When I walked past the nurses' station, two residents were rolling their eyes at each other, and I caught the tail end of their conversation: 'Another one thinks she's dying.' The charge nurse was already filling out transfer paperwork for psych. Nobody was rushing. Nobody looked concerned. I'd been at County General for six years, and I recognized this particular brand of dismissal immediately. They'd already decided what they were dealing with before examining her. I should have kept walking to my own patients—I had four charts waiting and a possible MI in bay three. But something about those screams made my skin prickle. They weren't incoherent. They were words, full sentences, pleading. When I glanced through the small window in her door, I saw a young woman gripping the bed rails, her knuckles white. I stepped into her room, and the look in her eyes told me something was very, very wrong.
 Image by FCT AI
Image by FCT AI
Practiced Indifference
Dr. Thompson walked past Marissa's room twice in the next twenty minutes, both times without stopping. I watched him do it. He's the kind of attending who's been practicing for so long that he's developed this sixth sense for which patients to take seriously—or at least, that's how he'd describe it. The rest of us had different words for it. The second time he passed, I actually stepped into the hallway and mentioned that the patient in twelve seemed coherent, that maybe we should run a basic panel. He glanced up from his tablet just long enough to give me that look—the one that said I was wasting his time with obvious things. 'Carter, she came in screaming about demons. Neighbor said she was out of her mind. Tox screen will come back positive, guarantee it.' His voice carried that practiced certainty that shuts down conversation. I opened my mouth to push back, but he was already moving toward the trauma bay where a car accident victim had just arrived. Real emergency. Real patient. I stood there feeling the familiar weight of institutional hierarchy pressing down. When I asked Thompson if we should run tests, he barely looked up from his chart.
 Image by FCT AI
Image by FCT AI
The Neighbor's Story
Later, during a rare quiet moment, I pulled up Marissa's intake notes on the computer. Rachel Kim, one of the newer nurses who hadn't yet learned to tune everything out, leaned over my shoulder. The paramedic's description was brief but vivid: 'Neighbor called 911 reporting female acting "possessed," screaming, clawing at her own head, speaking rapidly but coherently about severe head pain. Disoriented to time but oriented to person and place.' I read it twice. Rachel pointed at the screen. 'That doesn't sound like the usual stuff we see, does it?' I shook my head. Most drug cases came in either belligerent or sedated, paranoid or unconscious. This description had details that didn't fit the narrative everyone had already accepted. The neighbor had used the word 'possessed,' sure, but he'd also noted she was coherent. That she knew who she was. That she was specifically describing head pain, not hallucinations. I pulled up the neighbor's contact information—Marcus Webb, lived in the same building. He'd ridden with her in the ambulance. The neighbor's description didn't sound like drugs—it sounded like terror.
 Image by FCT AI
Image by FCT AI
Six Years of Rhythms
Six years in emergency medicine teaches you the unspoken rules faster than any textbook. You learn which attendings want to be consulted on every decision and which ones hate being bothered. You learn that the guy in a suit gets a warmer greeting than the guy in stained sweatpants, even if they're presenting with identical symptoms. You learn that certain words in a chart—'agitated,' 'uncooperative,' 'frequent flyer'—color every interaction that follows. I'd seen good doctors miss things because they'd been primed by a paramedic's offhand comment or a triage nurse's assessment. I'd done it myself. We all had. The ER runs on pattern recognition, and most of the time, that's what keeps people alive. You see a combination of symptoms and presentations enough times, your brain automatically slots new patients into familiar categories. It's efficient. It's necessary. And sometimes, it's catastrophic. I'd learned when to push and when to let go, when to trust my gut and when to defer to more experienced physicians. I'd learned the careful dance of raising concerns without seeming difficult. But this time, something held me back from walking away.
 Image by FCT AI
Image by FCT AI
Marcus at the Door
Marcus Webb showed up at the nurses' station around eight PM, still wearing his warehouse uniform, asking about the woman he'd brought in. Rachel pointed him toward me, and I took him to the small consultation room near the vending machines. He was early forties, tired-looking, but his eyes were sharp and concerned. 'How is she? Marissa—is she okay?' I asked him to walk me through what he'd seen. He'd lived across the hall from her for about a year, he said. They were friendly, said hello in the mornings. That afternoon, he'd heard screaming through the walls. 'At first I thought maybe she was on the phone, having an argument or something. But it didn't stop. And the things she was saying—she kept screaming about her head splitting open, about pressure. I knocked, and when she opened the door, I barely recognized her.' His hands moved as he talked, demonstrating. 'She looked terrified. Absolutely terrified. But she knew who I was. She asked me to call 911. She said please.' He paused, his expression darkening. 'He said she'd been holding her head like something inside was trying to get out.
 Image by FCT AI
Image by FCT AI
The Pupil Test
I went back to Marissa's room with a penlight and the excuse that I was checking her vitals. She'd finally stopped screaming but she was breathing hard, both hands pressed to her temples. The fluorescent lights made her skin look gray. 'Marissa, I'm Dr. Carter. I need to do a quick exam, okay?' She nodded, and I noticed her hands were trembling. I started with the basics—reflexes, coordination, pupil response. Her speech was pressured but coherent when she answered my questions. She knew the date, the president's name, where she was. Not drugs, my brain kept repeating. This isn't drugs. Then I shone the light in her eyes. The right pupil constricted normally, a perfect brisk response. I moved to the left. Watched. Waited for the familiar contraction. It came, but slower. Weaker. I tested again to be sure, checking both pupils multiple times. The asymmetry was subtle—the kind of thing you'd miss if you weren't looking for it, if you'd already decided what you were seeing. But it was there. Definitive. My stomach dropped. One pupil responded normally—the other didn't.
 Image by FCT AI
Image by FCT AI
Please Don't Let Them Ignore Me
I was still holding the penlight when Marissa's hand shot out and grabbed my wrist. Her grip was surprisingly strong. 'Please,' she said, and her voice cracked. 'Please don't let them ignore me.' I looked down at where her fingers pressed into my skin, then back at her face. Tears were streaming down her cheeks. 'I can feel it. Something's really wrong. I'm not—I've never—' She struggled for words. 'I don't do drugs. I don't drink. Something is wrong with my head and everyone keeps walking past like I'm crazy.' The desperation in her voice cut through every professional boundary I'd been trained to maintain. She was begging. Actually begging not to be dismissed, not to be categorized and forgotten. I thought about Thompson's confident dismissal, about the eye-rolls at the nurses' station, about how easy it would be to just accept the narrative everyone else had already written. How much easier my shift would be if I just let this go. But I couldn't. The way she looked at me—like I was her last chance—made it impossible to walk away.
 Image by FCT AI
Image by FCT AI
The Brother Arrives
David Chen burst through the ER entrance around nine-thirty, nearly running to the registration desk. I heard the commotion and walked over just as he was saying his sister's name. He looked frantic, his shirt untucked, car keys still in his hand. 'Where is she? Where's Marissa? They called me and said she was brought in for drugs, but that's impossible. My sister doesn't even take aspirin.' Rachel appeared beside me and quietly confirmed the room number. I introduced myself and asked David to step aside for a moment. 'Tell me about your sister. Any medical history I should know about?' He shook his head rapidly. 'Nothing. She's healthy. She runs marathons. She's a teacher, for god's sake. She's the most stable person I know.' His voice was rising. 'And she's never touched drugs. Never. Whoever told you that is lying or confused or—' He stopped mid-sentence, fumbling for his phone. 'Look, I saw her three days ago. Three days.' He pulled out his phone and showed me a photo of Marissa from just three days earlier—she looked completely different.
 Image by FCT AI
Image by FCT AI
Pushback
I found Dr. Thompson in the physician's lounge around ten-fifteen, typing notes on his laptop. I'd already rehearsed what I wanted to say—calm, professional, evidence-based. 'I need to talk to you about the patient in Bay Seven,' I started. 'Marissa Chen. I really think we need imaging.' He didn't look up from his screen. 'We've already discussed this, Dr. Carter.' His tone was flat, dismissive. I pressed on anyway. 'Her brother showed me a photo from three days ago. She looked completely different. And her symptoms don't fit recreational drug use—there's focal neurological involvement, the headache pattern is all wrong, and—' He finally looked at me, and I saw the irritation in his eyes. 'I've been doing this for twenty-three years,' he said slowly, like he was explaining something to a child. 'I know what a drug case looks like. You're still learning to trust your clinical judgment, and that's fine, but I'm not ordering expensive imaging on every patient who comes in altered.' I stood there, holding my ground, feeling my face get hot. He told me I was wasting resources on a patient who 'just needed to sleep it off.'
 Image by FCT AI
Image by FCT AI
History's most fascinating stories and darkest secrets, delivered to your inbox daily.
The Slurred Speech
When I went back to check on Marissa around eleven, Rachel was already in the room, adjusting her IV. I noticed it immediately—Marissa's speech had changed. 'The prrrressure,' she said, her words sliding together. 'It's like... spreading. Down my neck now.' Her eyes were focused, frightened, but her mouth wasn't cooperating properly. Rachel caught my eye, and I saw my own concern reflected back. I sat down on the edge of the bed. 'Can you describe where you feel it?' Marissa's hand moved slowly to the back of her head, then traced a path down toward her shoulder. 'Started here. Now it's... it's moving. Or growing. I don't know which.' She was trying so hard to articulate what was happening inside her skull. I checked her pupils again—still reactive, but slower on the left. Rachel handed me the penlight without me asking. 'How's the headache now? Same, better, worse?' Marissa closed her eyes. She whispered that it felt like something was crawling through her brain.
 Image by FCT AI
Image by FCT AI
The Chart Review
I pulled Marissa's chart and sat down at the nurses' station to actually read through everything properly. Sometimes in the chaos of the ER, you rely on what you're told during handoff, what gets shouted across the room. But I needed to see it all myself. The intake forms were straightforward—no history of drug use documented anywhere. No psychiatric hospitalizations. No previous ER visits for altered mental status. Her emergency contact was David. Her primary care physician was listed, someone in Westwood. Under the social history section: 'Patient reports no tobacco use, occasional alcohol (1-2 drinks per month), no recreational drug use.' The paramedic report mentioned confusion and agitation, but nowhere did it actually say they'd found drugs or paraphernalia. They'd been called because a colleague found her disoriented in her classroom after school. That was it. That was the entire basis for the assumption. I flipped back through the triage notes, the nursing assessment, the preliminary exam notes. Every line contradicted the assumption everyone had made within minutes of her arrival.
 Image by FCT AI
Image by FCT AI
Calling in the Specialist
I stepped outside the ER entrance to make the call, away from Dr. Thompson and anyone who might report back to him. I'd met Dr. Anita Patel at a case conference six months earlier—she was brilliant, direct, and didn't tolerate bullshit. My hands were shaking slightly as I dialed her mobile number. She answered on the third ring. 'Dr. Patel, this is Alex Carter from the ER at Metropolitan. I'm sorry to call you directly, but I have a thirty-six-year-old woman presenting with severe headache, confusion, visual disturbances, and now slurred speech. Progressive symptoms over several hours. No history of substance abuse despite initial assessment.' I heard her shift the phone. 'Imaging?' she asked. 'That's the problem,' I said. 'My attending won't order it. He's convinced it's a drug case, but nothing fits that picture. Her brother brought in a photo from three days ago—she looked completely normal. This is acute, and it's getting worse.' I described the focal deficits, the pattern of the headache, the maintained awareness despite the hallucinations. Dr. Patel's silence on the other end of the line lasted just long enough to make my stomach drop.
 Image by FCT AI
Image by FCT AI
The Hallucinations Intensify
Around eleven-forty, David called me back into Marissa's room. She was sitting up now, both hands pressed against her temples, staring at the corner of the ceiling. 'They're back,' she said quietly. 'The lights. But now there are... shapes. Geometric patterns, like... tessellations? Moving across my vision.' Her voice was still slurred, but she was so precise in her description. David looked at me desperately. 'What's causing this? Please, just tell me what's happening to her.' I didn't have an answer yet, not one I could confirm. Marissa turned toward me, her eyes tracking something I couldn't see. 'There—did you see that flash? Like lightning but inside my head.' She blinked hard. 'I know they're not real. I know I'm the only one seeing them. That means something's really wrong with me, doesn't it?' She was crying now, tears running down her face while she catalogued her own symptoms with the analytical mind of someone who'd spent her life teaching others to think clearly. The fact that she could describe them so precisely while they were happening made it worse, not better.
 Image by FCT AI
Image by FCT AI
The CT Finally Happens
Dr. Patel arrived at the hospital around twelve-thirty and went straight to Dr. Thompson. I don't know exactly what she said, but twenty minutes later, the CT order finally appeared in the system. Rachel and I got Marissa ready for transport. She was worse now—the slurring more pronounced, her left hand trembling when she tried to sign the consent form. 'Finally,' David breathed when I told him. 'Finally someone's taking this seriously.' The transport team arrived with the gurney. Marissa looked so small suddenly, vulnerable in a way that made my chest ache. I helped Rachel transfer her over, making sure the IV lines were secure. 'I'm going down with you,' I told Marissa. She nodded, or tried to. Her movements were becoming less coordinated. The hallucinations were still happening—I could tell by the way her eyes tracked invisible objects. As they wheeled her down the corridor toward radiology, the fluorescent lights harsh overhead, she reached out and grabbed my hand with surprising strength. Her fingers were ice cold. She asked if I thought she was crazy.
 Image by FCT AI
Image by FCT AI
The Image on the Screen
The images started appearing on the screen in radiology, slice by slice. I was standing next to Dr. Patel, and I heard her sharp intake of breath before I fully understood what I was seeing. Then it came into focus—a massive, irregular mass in Marissa's right frontal lobe, extending into the temporal region. It was huge, pressing against surrounding structures, causing visible midline shift. The edges were poorly defined, suggesting aggressive growth. Dr. Patel zoomed in on one section, her face grim. 'Glioblastoma, most likely,' she said quietly. 'Look at the necrotic center. The enhancement pattern. Jesus Christ, this is advanced.' Behind us, I heard someone page neurosurgery. James Larson, one of the neurosurgeons, appeared within minutes—he must have been in the hospital already. He stood beside us, studying the images without speaking. I watched him trace the tumor's borders with his eyes, calculating, assessing. Nobody said anything for what felt like a full minute. My mind was racing—how long had this been growing? How had she been functioning normally three days ago? I stared at the screen, and for the first time in my career, I couldn't find words.
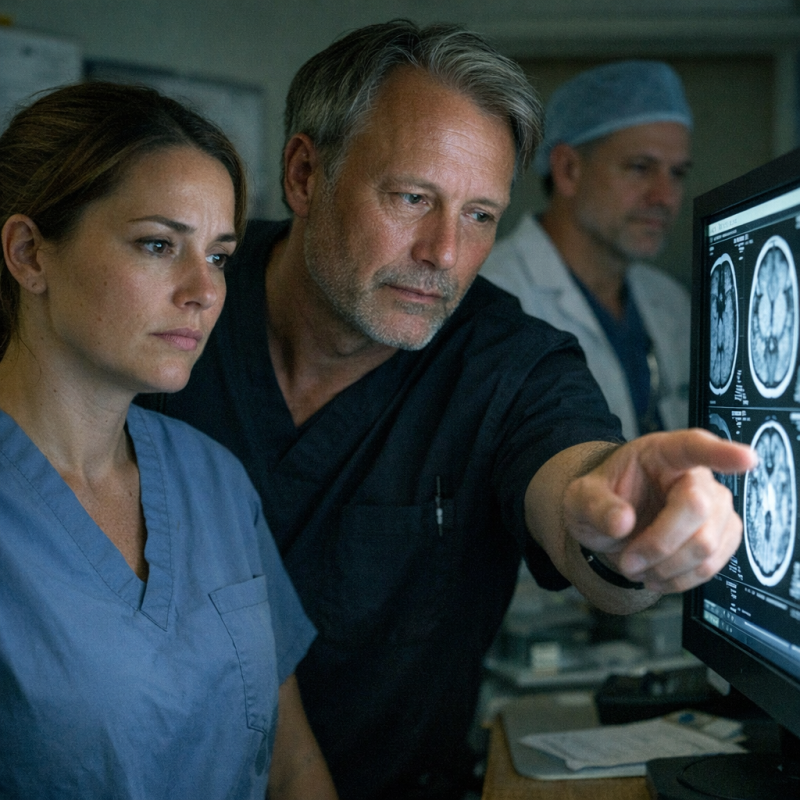 Image by FCT AI
Image by FCT AI
Thompson's Face
Dr. Thompson appeared in the radiology reading room about ten minutes after the images came up. Someone must have paged him. I was still standing there with Dr. Patel and Dr. Larson, all of us processing the magnitude of what we were looking at. Thompson walked up to the monitor, glanced at the images, and I watched his expression transform in real time. The dismissive confidence drained from his face. His jaw tightened. He leaned closer to the screen, as if proximity might somehow change what was displayed there. 'This is the patient from Bay Seven?' he asked, though he obviously knew the answer. Dr. Patel nodded curtly. 'The one Dr. Carter called me about. The one who needed imaging three hours ago.' Her voice was pointed, professional, but the subtext was clear. Thompson's eyes flicked to me briefly, then back to the screen. His hand came up to his chin—a defensive gesture, I noticed. He stood there in silence while Dr. Larson outlined the surgical approach they'd need to take, the urgency of decompression, the poor prognosis given the size and location. He opened his mouth to say something, then closed it again, and I realized he had no excuse.
 Image by FCT AI
Image by FCT AI
Telling Marissa
I went to Marissa's room after they'd moved her upstairs, David sitting in the chair beside her bed. The words felt like stones in my mouth. I pulled up a stool and sat at her level, not standing over her, and explained what the MRI showed—a large mass in her frontal lobe, likely causing all her symptoms. Her face went through so many expressions I couldn't track them all. Relief. Vindication. Terror. David reached for her hand. 'Is it cancer?' she asked, and I told her we wouldn't know until biopsy, but regardless, it needed to come out. She nodded slowly, processing. 'I knew something was wrong,' she said, her voice breaking. 'I kept telling them I wasn't on drugs. I kept saying it wasn't withdrawal.' I wanted to apologize for every minute she'd spent being doubted, but the words felt inadequate. David was crying quietly, squeezing her hand. Marissa looked at me with this expression I'll never forget—not anger, just exhausted validation. She closed her eyes, and tears slid down into her hair as she whispered, 'I told them.'
 Image by FCT AI
Image by FCT AI
The Administrator's Office
Dr. Susan Michaels' office was on the administrative floor, all polished wood and framed credentials. She'd called me up there the next morning, her tone neutral on the phone but deliberate. When I walked in, she gestured to a chair across from her desk and closed the door behind me. 'I've been reviewing the Chen case,' she said, folding her hands on the desk. 'Walk me through the timeline.' I did, carefully, watching her face stay professionally blank as I described the initial presentation, Dr. Thompson's assessment, the hours that passed. She took notes on a legal pad, underlining certain phrases. 'And you ordered the imaging?' she asked. I nodded. 'After consulting Dr. Patel.' She looked up at me then, and I saw the calculation happening behind her eyes—liability, exposure, institutional risk. Not malice, exactly, but the cold math of potential lawsuits. She asked how long Marissa had been in the ER before imaging was ordered, and I told her the truth.
 Image by FCT AI
Image by FCT AI
The Surgical Consult
Dr. Larson met with us in a quiet consultation room—me, Marissa, and David. He had a tablet with the MRI images, and he walked through them methodically, showing the tumor's position and size. His manner was calm but unflinchingly honest, the way good surgeons are when the odds aren't great. 'It's operable,' he said, 'but the location makes it complicated. It's pressing against areas that control motor function, some language processing, personality regulation.' Marissa listened with this intense focus, David translating the medical jargon when she looked confused. Dr. Larson explained the approach, the craniotomy, the microsurgical technique they'd use. Then he laid out the risks: bleeding, stroke, infection, neurological deficits that might be temporary or permanent. 'What if you don't operate?' David asked. Dr. Larson's expression didn't change. 'Then the tumor continues growing, and the outcome is certain.' Marissa nodded slowly, understanding. He said the tumor was operable, but the location meant there were no guarantees.
 Image by FCT AI
Image by FCT AI
Rachel's Confession
Rachel found me in the break room two days before Marissa's surgery, coffee in hand, looking like she'd been working up the nerve to say something. I could tell from her body language—that hesitant approach nurses get when they're about to cross a professional line. She sat down across from me and stared at her coffee for a moment. 'I need to tell you something,' she said quietly. 'About what happened with Marissa.' I waited. 'I've seen this before,' she continued. 'Not exactly this, but... patients getting dismissed when they probably shouldn't be. I've felt it, that instinct that something's off, but I didn't push back.' Her voice was tight with guilt. 'Why not?' I asked, not accusingly, just curious. She looked at me directly then. 'Because we're trained not to. You know? There's this culture of not questioning the doctors, especially the attendings.' I thought about Thompson, about the power dynamics in medicine. She said there was a culture of not questioning the doctors, even when something felt off.
 Image by FCT AI
Image by FCT AI
The Night Before Surgery
I stopped by Marissa's room the evening before her surgery, technically off-shift but unable to stay away. David had gone home to shower and sleep, and she was alone, staring at the ceiling. 'Can't sleep?' I asked from the doorway. She smiled weakly. 'Would you?' I pulled up the chair David had been living in and sat. We talked about nothing important at first—bad hospital food, the noise of the IV pump, the weirdness of hospital time. Then she got quiet. 'I'm scared,' she admitted. 'I know,' I said. 'That's completely normal.' She turned her head to look at me. 'What if I wake up different? What if I don't wake up at all?' I didn't have good answers for those questions. No one did. 'Dr. Larson is one of the best,' I offered. She nodded, then asked something that caught me off-guard entirely. She asked if I believed in second chances, and I didn't know how to answer.
 Image by FCT AI
Image by FCT AI
The Social Worker's Files
Emily Rodriguez, one of the hospital social workers, caught me in the hallway outside Marissa's room. We'd crossed paths a few times during the admission—she'd been helping David navigate insurance issues and disability paperwork. 'This case,' she said, shaking her head. 'It's really got me thinking.' I asked what she meant. 'I had another patient, maybe six months ago? Similar situation. Young woman, came in with neurological symptoms, got labeled as drug-seeking.' She paused, remembering. 'The presentation reminded me so much of your patient.' My attention sharpened. 'What happened?' I asked. Emily's expression shifted, something closing off behind her eyes. She glanced down the hallway, then back at me. 'I don't remember all the details,' she said, but her tone suggested otherwise. 'Different outcome, I think.' I pressed gently, asking if the patient got appropriate imaging, appropriate care. When I asked what happened to that patient, Emily's face went very still.
 Image by FCT AI
Image by FCT AI
The Surgery
The surgery started at seven in the morning. David and I camped out in the surgical waiting area, that uniquely awful space with too-bright lighting and magazines from 2019. I'd brought my laptop, pretending I could focus on charting, but mostly I just refreshed my email and watched David pace. He'd get coffee, sit for ten minutes, then get up again. 'How long do these usually take?' he asked for the third time. 'Depends,' I said. 'Brain surgery is slow. Careful.' The updates came every ninety minutes or so—a nurse would appear, tell us things were proceeding as expected, then vanish again. I watched other families get news, good and bad, cycle through the waiting room. Three hours became four. Four became five. I kept thinking about Marissa's question about second chances, about belief. David had stopped pacing and was just sitting, statue-still, staring at nothing. Five hours in, Dr. Larson emerged from the OR, and I couldn't read his expression.
 Image by FCT AI
Image by FCT AI
Touch and Go
Dr. Larson still had his surgical cap on, the mask pulled down around his neck. He looked exhausted in that particular way surgeons do after long, complex cases. David stood up so fast he nearly knocked over his chair. 'She's alive,' Larson said immediately, and I watched David's knees nearly buckle with relief. 'We removed approximately eighty-five percent of the tumor. There was some infiltration into surrounding tissue we couldn't safely take without causing definite damage.' He explained the parts he could and couldn't access, the microsurgical decisions made in real-time. 'So it's good?' David asked. 'It's good,' Larson confirmed, 'but she's not out of the woods. The brain doesn't like being operated on. There's swelling, there's trauma to the tissue, and we won't know for a while how she'll recover neurologically.' I asked about function, about deficits. He hesitated. 'Too early to tell. She's in recovery now, still intubated.' He said the next forty-eight hours would tell us whether she'd wake up as herself.
 Image by FCT AI
Image by FCT AI
The ICU Vigil
I found myself in the ICU more than I needed to be those first two days. Not because Marissa was my patient anymore—she'd been transferred to Dr. Patel's service—but because I couldn't shake the feeling that I needed to see this through. She remained unconscious, the ventilator still breathing for her, her face swollen from surgery. The monitors beeped their steady rhythms. David was there constantly, talking to her like she could hear him. Rachel would catch me standing at the doorway and give me this knowing look that said she understood. On the second day, I was reviewing her vitals at the nurses' station when Rachel called me over. 'You should see this,' she said quietly. We walked to Marissa's bedside, and Rachel gently touched her hand. 'Marissa, can you squeeze my fingers?' I held my breath. Nothing at first. Then—so slight I almost missed it—her index finger twitched. Just once. 'There,' Rachel whispered. It wasn't much, barely anything really, but it was the first sign that she was still in there, fighting her way back. On the second day, her fingers moved—just slightly, but enough.
 Image by FCT AI
Image by FCT AI
The Other Patient
That evening, I couldn't stop thinking about what Emily had mentioned—the other patient she'd seen dismissed the same way. I logged into the hospital records system and started searching: young women, neurological symptoms, discharged from the ER in the past year. It took me almost an hour of filtering through cases before I found her. Jasmine Williams, twenty-eight years old. Presented with severe headaches, visual disturbances, confusion. Chief complaint documented as 'drug-seeking behavior.' Discharged with instructions to 'follow up with primary care and consider substance abuse treatment.' She'd returned to the ER three days later, unresponsive. Brain hemorrhage from a ruptured aneurysm. Dead within hours. I sat there staring at the screen, feeling sick. The parallels were impossible to ignore—the same dismissive language, the same assumptions, the same catastrophic outcome. I scrolled down to see who'd been working that shift, who'd made the call to send her home. The attending physician listed on that case was Dr. Gerald Thompson.
 Image by FCT AI
Image by FCT AI
Marissa Wakes
On day three post-op, they extubated her. I wasn't there when it happened, but David called me immediately. By the time I got to the ICU, Marissa was breathing on her own, her eyes open but unfocused. Dr. Patel was at her bedside, doing a neurological assessment. 'Marissa, do you know where you are?' Patel asked gently. There was a long pause. Then, in a voice so hoarse it was barely audible: 'Hospital.' David started crying. I hung back, trying to maintain some professional distance, but honestly I felt my own eyes burning. Patel continued the exam—she could move all her extremities, knew her name, knew David, could follow simple commands. The cognitive function was there. As I turned to leave, giving them privacy, I heard David say, 'That's Dr. Carter. She's the one who saved you.' Marissa's eyes found mine across the room. Her face was still swollen, half her head wrapped in bandages, but she was looking at me with such clarity. She looked at me and mouthed two words: 'Thank you.'
 Image by FCT AI
Image by FCT AI
The Question I Couldn't Ask
I thought about confronting Thompson maybe a dozen times over the next few days. I'd rehearse what I'd say in my head during my commute, in the shower, lying awake at three in the morning. But every time I saw him in the hospital, something stopped me. What exactly would I accuse him of? Making a diagnostic error? We all make those. Having implicit bias? He'd deny it, and I couldn't prove intent. The thing about doctors like Thompson is they're protected by plausible deniability. He could say he made a judgment call based on the information available. He could say Marissa's behavior seemed consistent with intoxication. He could say he was managing a busy ER with limited resources. And technically, on paper, he wouldn't be entirely wrong. That's what made it so insidious. On Thursday, I was walking past the doctors' lounge when I saw him pouring coffee, chatting with one of the attendings about golf. He looked relaxed, completely unbothered. I saw him in the hallway and froze, wondering if he even remembered that patient's name.
 Image by FCT AI
Image by FCT AI
David's Story
David caught me in the cafeteria on Friday. I was grabbing coffee between patients when he sat down across from me without asking. 'I wanted you to know who she is,' he said. 'Not just the patient you saved, but who Marissa actually is.' He told me about her work as a third-grade teacher, how she stayed late every day to help kids who were struggling. How she'd organized a fundraiser for a student whose family lost their home in a fire. How she volunteered at a literacy center on weekends. He showed me pictures on his phone—Marissa laughing with her students, Marissa at a protest march for teacher salaries, Marissa with their elderly parents at Christmas. 'She's the person who shows up,' David said quietly. 'For everyone. Always.' He paused, looking down at his coffee. 'And when she needed someone to show up for her, when she was in more pain than she'd ever been in her life, they treated her like garbage.' He said the worst part was knowing she'd been screaming for help and no one believed her.
 Image by FCT AI
Image by FCT AI
The Complaint
I met Emily in the hospital library—neutral territory, away from listening ears. She'd pulled some strings in her department and found something I wouldn't have had access to otherwise. 'There was a complaint filed against Thompson,' she said, sliding a folder across the table. 'Six months ago.' I opened it. A patient named Marcus Johnson had filed a formal grievance after his mother died from what turned out to be bacterial meningitis. She'd presented with fever, confusion, and agitation. Thompson had documented 'suspected methamphetamine intoxication' and recommended psychiatric evaluation. By the time someone realized she had an infection, it was too late. The son's complaint was detailed, anguished, specific. He outlined everything Thompson had said, the assumptions made, the dismissive treatment. There was a response from the hospital's quality review committee attached. I read it twice to make sure I was understanding correctly. The complaint had been reviewed and dismissed as 'unsubstantiated.'
 Image by FCT AI
Image by FCT AI
Rachel's Warning
Rachel pulled me aside after morning rounds. We ended up in the med room, the one place we could talk without being overheard. 'I heard you've been asking questions about Thompson,' she said, her voice low. Word traveled fast in hospitals—someone must have seen me in the library with Emily, or noticed me accessing old cases. 'I'm just trying to understand what happened with Marissa,' I said. Rachel shook her head. 'I get it, I really do. But you need to be careful.' She told me about a physician assistant who'd reported a senior doctor for similar issues two years ago. The PA had been systematically frozen out—excluded from procedures, given terrible schedules, eventually pressured into leaving. 'The hospital protects its own,' Rachel said. 'Especially the attendings who bring in revenue and don't make waves with insurance companies.' I told her I couldn't just let it go, not after what I'd seen. She looked at me with something like pity. She said people who make waves don't last long here.
 Image by FCT AI
Image by FCT AI
Marissa's Progress
By the end of the week, Marissa had started therapy. I stopped by to see how she was doing and found her in the rehab gym with a physical therapist, working on balance exercises. She was shaky, holding onto parallel bars, but she was standing. Dr. Patel was there too, observing. 'Her progress is remarkable,' Patel told me quietly. 'Honestly, given the size of that tumor and how long it went untreated, this is the best-case scenario.' Marissa saw me and waved me over. Her speech was still slightly slurred, and she tired easily, but her mind was sharp. We talked about her recovery timeline, about the follow-up treatments she'd need. Then she said something that caught me off guard. 'I've been thinking about what happened to me,' she said. 'How many times I was ignored, how close I came to dying because no one would listen.' She gripped the parallel bar tighter. 'I want to do something about it. I don't know what yet, but something.' She told me she wanted to make sure no one else went through what she did.
 Image by FCT AI
Image by FCT AI
The Meeting with Michaels
Dr. Michaels called me to her office three days after Marissa started therapy. I thought maybe it was going to be a congratulations, a 'job well done' conversation. I was wrong. She had a document waiting on her desk, typed up all official-looking with legal letterhead. She slid it across to me and asked me to read it and sign. It was a statement about Marissa's case, describing the diagnostic delay as 'unfortunate but understandable given the complexity of presentation and initial physical examination findings.' It said that all protocols were followed and that the ER team made 'clinically reasonable decisions based on available information at the time.' I read it twice. There was no mention of the dismissiveness, the refusal to order imaging, the assumption that she was drug-seeking. It was clean, sanitized, protective. 'This is for the quality review committee,' Michaels said. 'Just a formality.' Her tone was casual, but her eyes were watching me carefully. I looked at the document and realized they were trying to make this disappear.
 Image by FCT AI
Image by FCT AI
The Third Case
I didn't sign it. I told Michaels I needed time to think, which bought me maybe a day or two. That afternoon, Emily Rodriguez showed up at my office looking uncomfortable. She closed the door behind her and sat down without being invited. 'I've been doing some digging,' she said. 'Going through old case files from patients I worked with.' She pulled out a folder with notes she'd compiled. There was another case, she told me, from two years ago. A young Black woman, twenty-eight, came in with severe headaches and confusion. Same pattern: dismissed as intoxicated, sent home with instructions to sleep it off. She came back three days later, comatose. Brain hemorrhage from an undiagnosed aneurysm. Emily's voice got quiet when she told me the rest. They'd done everything they could, but the damage was too extensive. The woman had been in the ICU for a week before her family made the decision to withdraw life support. That patient didn't survive.
 Image by FCT AI
Image by FCT AI
Looking for Allies
I reached out to Dr. Patel that evening. We met in the hospital cafeteria after her shift, somewhere neutral where we could talk without being overheard in an office. I told her about the third case, about the pattern I was seeing, about the document Michaels wanted me to sign. I asked her if she thought we should report this formally, maybe to the state medical board or the hospital ethics committee. Patel stirred her coffee for a long time before answering. 'Alex, I understand what you're feeling,' she said finally. 'I do. But I've been practicing for twenty years, and I've seen this play out before.' She told me about a colleague at her previous hospital who'd reported a pattern of surgical complications. The surgeon in question had connections, and the whistleblower ended up ostracized, eventually forced out. 'They'll protect the institution first,' Patel said. 'Always.' She wasn't saying no, exactly, but she wasn't saying yes either. Dr. Patel said she'd seen things like this before, and it never ends well for the whistleblower.
 Image by FCT AI
Image by FCT AI
The Demographics
That night, I couldn't sleep. I kept thinking about the three cases: Marissa, the woman with the aneurysm, and even Jackson's overdose that I'd brushed off at first. I pulled out my notes and laid them side by side on my kitchen table. Marissa Chen: Asian-American woman, presumed drug-seeking. The woman with the aneurysm: young Black woman, presumed intoxicated. Jackson: white male, actually was using, but even I'd made assumptions before really looking. Then I thought about the other dismissals I'd witnessed over the years, the patients who seemed to get less benefit of the doubt. I started writing down what I remembered: their demographics, their complaints, how they'd been treated. A pattern emerged that made my stomach turn. All three documented cases involved women or minorities who were dismissed as drug users. The ER doctors—Dr. Thompson especially—had made assumptions based on who these patients were, not just what they were saying. The pattern wasn't just medical—it was who was being ignored.
 Image by FCT AI
Image by FCT AI
Marissa Learns the Truth
I went to see Marissa during her afternoon physical therapy session. She was walking with a cane now, doing better every day. I asked if we could talk privately, and her therapist gave us the room. I sat down and told her everything: about the woman who'd died two years ago, about the pattern of dismissals, about patients being sent home because doctors assumed they were drug-seeking based on appearance and demographics. Marissa listened without interrupting, her jaw getting tighter with every detail. 'So I'm not the only one,' she said finally. 'No,' I told her. 'You're not.' She was quiet for a moment, processing. I could see the anger building behind her eyes, but it was focused anger, purposeful. She'd been through an nightmare and survived, and now she was learning that her suffering was part of something bigger, something systemic. She looked at me directly, and I saw the steel I'd first glimpsed when she'd talked about wanting to do something. Marissa's expression hardened, and she said, 'Then we need to do something about it.'
 Image by FCT AI
Image by FCT AI
The File Request
I decided to go through official channels first. I submitted a formal request to medical records for access to patient files involving Dr. Thompson over the past three years, specifically cases with diagnostic delays or missed diagnoses in the ER. I cited quality improvement and patient safety as the reason, kept it professional and by-the-book. I figured it might take a day or two to process, maybe a week if they were being thorough. The request was submitted at nine in the morning. By ten, I had an email from Dr. Michaels asking me to come to her office. By ten-thirty, I was sitting across from her again, and she was not happy. 'This kind of fishing expedition requires committee approval,' she said, her voice tight. 'You can't just request confidential patient files without proper justification and oversight.' I explained my justification: patient safety, quality improvement, pattern recognition. She cut me off. 'Request denied,' she said. 'If you have specific concerns about a specific case, file an incident report through proper channels.' The request was denied within an hour.
 Image by FCT AI
Image by FCT AI
Rachel's Records
Rachel found me in the stairwell two days later. She looked around to make sure we were alone, then pulled a manila folder from under her scrubs. 'I heard about your request getting denied,' she said quietly. 'I figured you might want to see these anyway.' She'd made copies of intake logs from the ER, going back three years. They weren't full patient files, just the initial nursing assessments and doctor's notes from triage. But that was enough. I could see the patterns in the handwriting alone: 'Patient appears intoxicated,' 'Suspected drug-seeking behavior,' 'Recommending discharge with referral to addiction services.' Case after case, dismissed before any real workup was done. 'This could get you in trouble,' I told Rachel. She shrugged. 'So could doing nothing.' I asked her why she was taking this risk, and she told me she'd been watching these dismissals happen for years, had advocated for patients and been overruled. 'Someone has to care,' she said. She handed me the folder and said, 'If anyone asks, you didn't get this from me.'
 Image by FCT AI
Image by FCT AI
The Pattern in Black and White
I spent that entire evening going through Rachel's copies. The intake logs covered three years of ER admissions, and she'd highlighted the cases that matched the pattern: patients who came in with neurological symptoms, were presumed to be intoxicated or drug-seeking, and were either discharged or admitted only after significant delay. I found seven cases that fit. Seven people who'd been dismissed, who'd had to fight to be taken seriously, who'd suffered because the first response was assumption rather than investigation. I cross-referenced them with outcomes where I could find the information. Two had died. Three had permanent disabilities. Two, including Marissa, had survived with successful treatment after the delay. I made a chart, listing demographics, presenting complaints, initial assessments, outcomes. The pattern was undeniable when you saw it laid out like that. Every single one involved a woman or person of color, and every single one was handled by Dr. Thompson.
 Image by FCT AI
Image by FCT AI
The Choice
I sat at my kitchen table for hours that night, staring at the chart I'd made. The data was there, undeniable, printed out in black and white. Seven cases. Two deaths. A pattern so clear it felt obscene that no one had acted on it before. I knew what filing a formal complaint would mean. I'd seen it happen to other doctors who'd challenged attendings, who'd questioned protocols, who'd made waves. They got shuffled to night shifts, passed over for promotions, quietly pushed out until they left on their own. My career at this hospital would effectively be over. Maybe my career anywhere, if Thompson had the connections people said he did. I'd spent eight years training for this. Medical school, residency, the brutal hours, the debt I was still paying off. Everything I'd worked for could disappear because I refused to look the other way. But then I kept coming back to that moment in the hallway, hearing Marissa scream while Thompson walked away. I thought about those two people who'd died, who'd never gotten a second chance. I thought about Marissa screaming in that room, and I knew I didn't really have a choice at all.
 Image by FCT AI
Image by FCT AI
The Report
I filed the complaint with the state medical board on a Tuesday morning. The online form asked for specifics, so I provided them—dates, patient identifiers, outcome summaries, the demographic breakdown that showed the clear bias. I attached my chart and the copies of intake logs Rachel had given me. My hands were shaking when I hit submit, but I did it anyway. The confirmation email arrived within minutes: 'Your complaint has been received and assigned case number MB-2019-4477. A board investigator will contact you within ten business days.' I saved the email, backed it up in three places, and forwarded a copy to my personal account. Then I went to work like it was any other shift. I saw patients, wrote orders, consulted with residents. No one knew what I'd just done. For about twenty-four hours, I almost convinced myself that maybe it would be handled quietly, professionally, without drama. That was naive. Within twenty-four hours, I was called into the hospital director's office.
 Image by FCT AI
Image by FCT AI
The Director's Threat
Director Morrison didn't ask me to sit down. He stood behind his desk with my complaint printed out in front of him, and his expression was the kind of cold I'd never seen directed at me before. 'Do you understand what you've done?' he asked. I told him I'd reported a pattern of medical negligence, which was my obligation. He laughed, but there wasn't any humor in it. He said I'd accused a respected physician of bias based on 'cherry-picked data and personal grievances,' and that the board complaint would trigger an investigation that would bring scrutiny to the entire department. He told me the hospital's legal team was already involved. Then he leaned forward and said that if I continued down this path, I should expect my contract not to be renewed. He mentioned that hospitals talk to each other, that references matter, that my 'judgment and professionalism' would be questioned everywhere I applied. The threat wasn't even subtle. He wanted me to withdraw the complaint, to apologize, to make this go away. I told him I wouldn't. He said I was making enemies I couldn't afford to have.
 Image by FCT AI
Image by FCT AI
David's Support
David called me two days after my meeting with Morrison. He said he'd heard through a friend who worked in hospital administration that there was tension around Marissa's case. I didn't know how much to tell him, but he didn't give me a choice. 'Whatever you're doing,' he said, 'whatever you're risking to hold them accountable—we're with you.' I tried to deflect, said I was just doing my job, but he cut me off. He told me that he and Marissa had already discussed it, that they knew standing up against the hospital meant putting my career on the line. 'If you need us to go public, we will,' he said. 'If you need witnesses, statements, anything—we're there.' His voice was steady, certain. He said Marissa wanted to help, that she'd been talking to a patient advocacy group. I felt something loosen in my chest, some tight knot of isolation I hadn't realized was there. He said his sister was alive because I refused to ignore her, and he wouldn't let them punish me for that.
 Image by FCT AI
Image by FCT AI
The Attorney's Call
The attorney's name was Sarah Mitchum, and she called me on a Thursday afternoon while I was between patients. She explained that medical board complaints were public record once they reached a certain stage, and that she'd been monitoring filings in the state. 'Your case caught my attention,' she said. 'The pattern you documented, the demographic breakdown—it's exactly the kind of systemic issue most people miss.' She asked if I'd be willing to meet, to discuss the complaint in detail. I was hesitant. I'd filed with the medical board, not looking to build a legal case. But she said something that made me pause: 'Dr. Carter, from what I'm reading, this isn't just about one doctor making bad calls. This is about an institution that let it happen.' She asked about hospital protocols, whether there'd been prior complaints, how administration had responded. I realized I didn't know the answers to most of her questions. I'd focused on Thompson, on the cases, on the pattern—but I hadn't thought about who else knew, who else had seen it and done nothing. She said if even half of what I documented was true, this was bigger than one doctor.
 Image by FCT AI
Image by FCT AI
The Anonymous Email
The email arrived from an address I didn't recognize: 'MercyGeneral47@protonmail.com.' No subject line. I almost deleted it as spam, but something made me open it. 'Dr. Carter,' it started, 'I'm a nurse who worked in the ED during the time period you documented in your board complaint. I can't identify myself yet, but I want you to know you're not wrong about Dr. Thompson.' The writer described three additional cases over the past two years—patients dismissed as intoxicated who later turned out to have serious medical conditions. One was a diabetic woman in DKA who Thompson insisted was just drunk. Another was a man with a subdural hematoma who'd been sent home and returned by ambulance six hours later, unconscious. The nurse wrote that they'd tried to advocate for these patients, had questioned the assessments, but Thompson had shut them down each time. 'I documented my concerns in incident reports, but nothing ever came of them,' the email continued. 'I thought about filing my own complaint, but I was scared of retaliation. I have a family, bills, a mortgage.' The email ended with: 'I was too afraid to speak up, but I'm glad you did.'
 Image by FCT AI
Image by FCT AI
The Hidden Complaints
Emily showed up at my apartment on a Saturday morning holding a manila folder that looked like it had been through a war. 'You need to see this,' she said, pushing past me into my living room. She spread documents across my coffee table—printouts of what looked like internal hospital forms, incident reports, and email chains. She explained that she'd been asking around, talking to social workers and nurses who'd been at the hospital longer than me. One of them had kept copies of complaints they'd filed years ago about patients being dismissed by Dr. Thompson. Emily had found five formal incident reports dating back three years, all documenting concerns about Thompson's assessments of marginalized patients. But when she'd cross-referenced them with the hospital's official records system, none of them appeared. They'd been filed, logged, and then—nothing. No investigations, no follow-up, no documentation that they'd ever existed. 'I found seven more through other staff,' Emily said, her voice shaking with anger. There weren't just three cases—there were at least twelve, and someone had buried every single one.
 Image by FCT AI
Image by FCT AI
The Truth About the System
Sarah Mitchum met me at a coffee shop off hospital grounds. She had her own folder now, thicker than Emily's had been. 'I've been deposing hospital staff as part of discovery,' she said. 'And I found something you need to understand.' She showed me email chains between Morrison and the hospital's risk management team, dating back two years. Multiple staff members had flagged Thompson's pattern of dismissing certain patients. The emails were clear: administrators knew. Risk management had even recommended 'enhanced oversight and unconscious bias training.' But Morrison had pushed back, arguing that formal action would create 'documentation that could be used against the hospital in litigation.' One email was particularly damning: 'If we acknowledge the pattern, we acknowledge institutional knowledge of the problem. Better to handle these as isolated incidents on a case-by-case basis.' They'd known for years. They'd had the data, the complaints, the warnings—and they'd actively chosen to protect Thompson to shield themselves from liability. It wasn't incompetence—it was a deliberate choice to protect the institution over patients.
 Image by FCT AI
Image by FCT AI
The Media Inquiry
Her name was Jennifer Walsh, and she showed up at my office without an appointment. She was an investigative reporter for the local public radio station, and she'd been following Sarah Mitchum's lawsuit filings. 'I've been looking at public records,' she said, settling into the chair across from my desk. 'Court documents, complaints to the medical board, patient advocacy groups. And I keep seeing the same name: Dr. Gerald Thompson.' She had a notebook filled with dates, cases, patterns. She'd talked to Emily Chen's family already. She knew about the emails Morrison had buried. 'What I'm seeing suggests this isn't just about one doctor,' she continued. 'This is about institutional negligence—a hospital that knew they had a problem and chose to hide it rather than fix it.' I felt my heart racing. Media exposure could force real change, but it could also paint a target on everyone who'd spoken up. 'I need to understand the medical side of this,' Jennifer said, her pen poised over her notebook. 'The pattern of who gets believed and who doesn't.' She asked if I was willing to go on the record.
 Image by FCT AI
Image by FCT AI
Marissa's Decision
I called Marissa before I made any decision. She deserved to know what was coming, to choose whether she wanted her story out there for everyone to dissect. David was with her when I arrived at their apartment, protective as always. 'A reporter wants to do a story,' I told them. 'About the pattern at the hospital. About what happened to you and Emily and the others.' Marissa was quiet for a long time, staring at her hands. She'd been through so much already—the dismissals, the near-death experience, the slow recovery. 'People will judge me,' she said softly. 'They'll say I was drug-seeking. They'll say I brought it on myself.' David reached for her hand, but she shook her head. 'But if I don't speak up, it keeps happening.' She looked at me then, her eyes clear and determined. 'How many people like me are out there right now, being told their pain isn't real?' I felt something shift in the room—courage taking root. She said if her voice could prevent even one person from being ignored, it was worth it.
 Image by FCT AI
Image by FCT AI
The Interview
The interview took place in Marissa's apartment. Jennifer set up a small camera while her producer adjusted the lighting. I sat off to the side, there for support if Marissa needed it. She was nervous—I could see her hands trembling slightly—but when the camera started rolling, she found her voice. She described every detail: the abdominal pain that had started suddenly, the ER visits where she'd been dismissed as drug-seeking, Thompson's refusal to order imaging despite her worsening symptoms. 'He looked at me like I was lying,' she said, her voice steady now. 'Like my pain was a performance.' She talked about the ruptured appendix, the sepsis, the weeks in the ICU wondering if she'd survive. 'I kept thinking, what did I do wrong? Why didn't they believe me?' Her voice cracked then, but she didn't stop. Jennifer leaned forward. 'What do you want people to know?' Marissa looked directly at the camera, and I saw something fierce in her expression. When the reporter asked what she wanted people to know, Marissa looked directly at the camera and said, 'Believe patients.'
 Image by FCT AI
Image by FCT AI
The Story Breaks
The story went live on a Tuesday morning. Jennifer had titled it 'Pattern of Dismissal: How One Hospital's Bias Nearly Cost Lives.' It was thorough—interviewing Marissa, citing Emily's case, referencing the buried emails, including responses from other patients who'd experienced similar dismissals. Sarah Mitchum had provided legal documentation. I'd given background on medical bias and diagnostic disparities. The piece was devastating in its clarity. By noon, it had been shared thousands of times on social media. Local news stations picked it up. National health reporters started calling the hospital for comment. I sat in my car during lunch, watching my phone explode with notifications—colleagues texting support, others asking if I knew what I'd done. David called to tell me Marissa's interview was trending. People were angry. They were sharing their own stories of being dismissed, ignored, labeled. The pattern wasn't just at our hospital—it was everywhere. Within hours, the hospital issued a statement denying everything—but the damage was done.
 Image by FCT AI
Image by FCT AI
The Suspension
Thompson was suspended two days after the story broke. Dr. Michaels made the announcement in a terse hospital-wide email: 'pending the outcome of an internal investigation into allegations of patient care concerns.' No mention of bias. No acknowledgment of the pattern. Just bland corporate language designed to minimize liability. I was in the ER when I saw him leaving the building, a cardboard box under his arm, his face stone. Rachel stood beside me at the nurses' station, watching through the window. 'Good riddance,' she muttered, but her voice lacked conviction. The hospital had also announced the formation of a 'patient care review committee' to examine triage protocols and implement 'enhanced training opportunities.' It sounded impressive in the press release. But I'd been in medicine long enough to know the difference between accountability and damage control. Thompson would probably land at another hospital within months. The review committee would issue recommendations that gathered dust on Morrison's desk. But as I watched him leave the building, I wondered if this would change anything at all.
 Image by FCT AI
Image by FCT AI
The Other Victims Come Forward
Jennifer's report had opened a floodgate. Within a week, she'd been contacted by seventeen families—people whose loved ones had been dismissed by Thompson or other physicians at the hospital. Some had survived, like Marissa. Others hadn't. I met with several of them at Jennifer's request, providing medical context where I could. There was Marcus Williams, who'd presented with crushing chest pain and been told it was anxiety. He'd had a heart attack in the parking lot. There was Diana Reeves, sent home with 'menstrual cramps' that turned out to be ovarian torsion. She'd lost the ovary. Each story followed the same pattern: pain dismissed, symptoms minimized, legitimate concerns labeled as exaggeration or drug-seeking. Jennifer was building a database, documenting everything. One afternoon, a mother named Patricia showed me a photo of her daughter, Keisha, who'd died at twenty-three from an infection that could have been treated if anyone had listened. 'She kept calling for help,' Patricia said, her voice breaking. 'She told them something was wrong. And they acted like she was bothering them.' One mother said her daughter had died calling for help, and no one listened—until now.
 Image by FCT AI
Image by FCT AI
The State Investigation
The state medical board showed up three weeks after the story broke. Two investigators in dark suits, carrying briefcases and official credentials. They set up in a conference room and started interviewing staff, reviewing charts, requesting documentation that Morrison had probably hoped would never see daylight. I was called in on a Thursday afternoon. They asked about Thompson's pattern, about the cases I'd flagged, about the institutional response when I'd raised concerns. I told them everything—the dismissed patients, the buried complaints, the emails showing administrators had known for years. They took notes without expression, professional and thorough. One investigator asked if I believed the hospital had acted in good faith. I thought about Morrison's office, his careful legal language, his priority of protecting the institution over patients. 'No,' I said simply. 'They knew there was a problem, and they chose to hide it.' The investigator nodded, making another note. As I left the conference room, I felt something I hadn't felt in months. For the first time, I felt like someone with real power was paying attention.
 Image by FCT AI
Image by FCT AI
The Policy Changes
The hospital announced the new protocols at a mandatory staff meeting. Dr. Michaels stood at the podium, reading from prepared remarks about 'patient-centered care initiatives' and 'comprehensive bias recognition training.' All ER patients would now be evaluated using standardized pain assessment tools. Physicians would complete quarterly training on implicit bias and diagnostic disparities. Patient advocates would be available for anyone who felt their concerns weren't being heard. It looked good on paper—impressive bullet points for the press release, concrete steps the hospital could point to when journalists asked what had changed. Some of my colleagues seemed genuinely hopeful. Rachel squeezed my arm as we filed out of the auditorium. 'This is what you fought for,' she whispered. And maybe it was. But I'd seen too many policy announcements that never translated into actual practice, too many training sessions that became box-checking exercises. Real change required more than revised protocols—it required a fundamental shift in how we saw patients, how we valued their voices. It was a start, but I knew words on paper weren't the same as real change.
 Image by FCT AI
Image by FCT AI
Marissa's Recovery Milestone
Dr. Patel delivered the news in her characteristically calm manner, but her eyes were bright. 'Scans are clear. Complete response to treatment.' Marissa sat perfectly still for a moment, then her shoulders started shaking with silent tears. David grabbed her hand. I'd seen them through so many appointments—the good updates and the terrifying setbacks—that this moment felt almost surreal. We'd gone from a patient dismissed as drug-seeking to a woman who'd fought cancer and won. The irony wasn't lost on any of us. Rachel had joined us for the appointment, squeezing into the small consultation room because she'd been part of this journey from that first screaming night in the ER. 'You did everything right,' Dr. Patel told Marissa. 'You advocated for yourself when it mattered most.' But as we stood to leave, Marissa turned to me, her face still wet. She wrapped her arms around me in a tight embrace that said more than any medical report could capture. She hugged me and whispered, 'We did it—both of us.'
 Image by FCT AI
Image by FCT AI
Six Months Later
Six months after that staff meeting, the hospital looked the same from the outside. Same fluorescent lights, same overcrowded waiting rooms, same exhausted residents grabbing coffee at 3 AM. But small things had shifted. I'd watched colleagues pause before dismissing a patient's pain, seen nurses pull doctors aside to say 'I think we should listen to this more carefully.' The quarterly training sessions happened, though some people clearly resented the time away from clinical work. The patient advocates were actually being utilized—not perfectly, not universally, but more than before. We still had cases where bias crept in, where assumptions overrode evidence. I still fought battles that shouldn't need fighting. But the conversation had changed. When I raised concerns now, people didn't automatically get defensive. Marissa's case had become part of our institutional memory, a cautionary tale referenced in teaching rounds. Some changes were measurable—documented reductions in pain assessment disparities, improved patient satisfaction scores. Others were harder to quantify but just as real. The work wasn't finished, but at least now, people were paying attention.
 Image by FCT AI
Image by FCT AI
The New Protocol in Action
The young Black woman came in complaining of severe abdominal pain. Before the new protocols, I could imagine exactly how this might have gone—skeptical looks, drug screen ordered first, assumption of exaggeration. But Rachel used the standardized assessment tool without hesitation, documenting objective findings alongside the patient's self-reported pain level. The attending physician, one who'd been notably resistant during training, actually listened to the full history before forming conclusions. He ordered appropriate imaging within the first hour. We found appendicitis before it ruptured—a straightforward diagnosis that might have been dangerously delayed under the old patterns of dismissal. The patient never had to scream to be heard. She never had to watch us exchange those knowing glances that said 'here we go again.' Her pain was treated, her concerns validated, her body given the same urgent attention we'd automatically give to patients who fit different demographics. It wasn't revolutionary medicine—it was basic competent care. But that's exactly what had been missing before. This time, the patient was believed from the start, and it made all the difference.
 Image by FCT AI
Image by FCT AI
Believing Patients
Marissa and I met for coffee near the hospital, though she wasn't a patient anymore. She looked healthy, her hair grown back, her color good. We talked about her plans to volunteer with cancer support groups, her brother's relief that life was returning to normal. Then she asked about the hospital changes, whether they were really working. I gave her the honest answer—that it was complicated, that progress was uneven, that some days felt like steps backward. 'But people are trying now,' I told her. 'That first night, nobody wanted to believe you were anything but an addict looking for a fix. Now we have systems pushing back against those assumptions.' She nodded slowly. 'I keep thinking about all the people who weren't as lucky as me. Who didn't have someone willing to push back.' That thought haunted me too. How many Marissas had we missed? How many were we still missing? We finished our coffee and hugged goodbye on the sidewalk. As I left the coffee shop, I thought about that first scream echoing down the corridor—and how many voices I'd heard since that finally weren't being ignored.
 Image by FCT AI
Image by FCT AI